A hospital deploys a model to screen scans for a serious tumor, and missing an actual tumor case (letting it go undetected) is far more dangerous than sending a healthy patient for an unnecessary follow-up. Which metric should this team prioritize?
Select an answer to reveal the explanation.
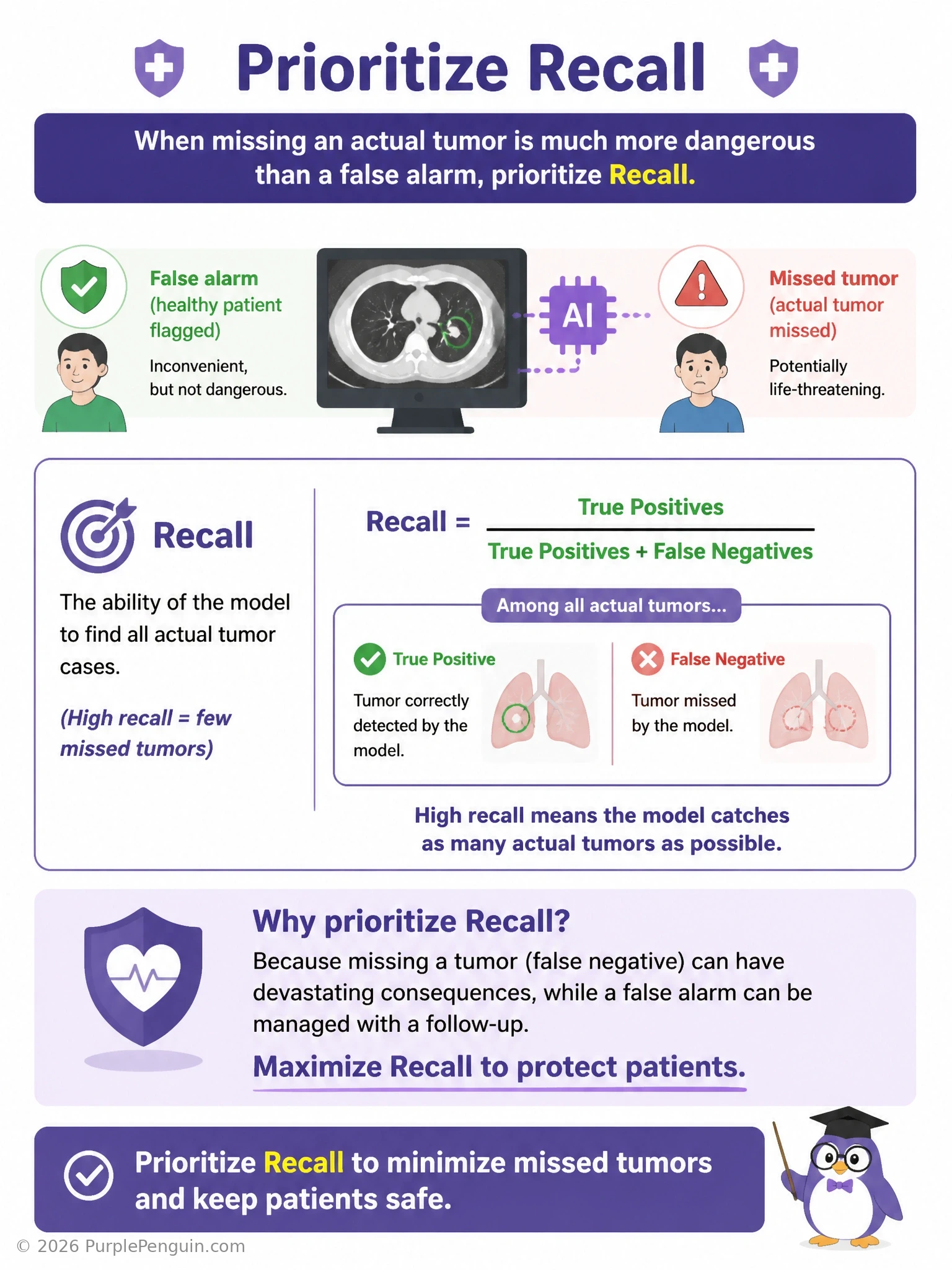
Short Explanation and Infographic
This is the textbook case for recall. When missing an actual positive case is the scary outcome — here, a real tumor slipping through undetected — you need the metric that's specifically built to measure how many of the true positive cases you actually caught. That's recall: true positives divided by true positives plus false negatives. High recall means very few tumors are getting missed, even if it means flagging some healthy patients for extra follow-up along the way. That's answer D. Precision is the wrong focus here because precision cares about false positives, meaning how many of your positive flags were correct — that's a real concern for reducing unnecessary follow-ups, but it's not the primary danger described. Specificity measures how well you correctly identify actual negatives, which again isn't the life-threatening concern here. And mean absolute error is a regression metric entirely unrelated to this yes/no screening decision.
Full explanation below image
Full Explanation
Recall (also called sensitivity or the true positive rate) is calculated as true positives divided by the sum of true positives and false negatives. It measures the proportion of all actual positive cases that the model successfully identified. When missing a true positive carries severe consequences — such as a tumor going undetected and untreated — recall is the metric that directly rewards minimizing false negatives, since a high recall score means the model is catching nearly all real positive cases, even if that comes at the cost of some false alarms on healthy patients.
Precision is incorrect as the priority here because it measures true positives divided by true positives plus false positives, focusing on how trustworthy a positive prediction is rather than how many actual positives were found; precision matters more when a false alarm (unnecessarily worrying or inconveniencing a healthy patient) is the primary cost to avoid, which is a secondary concern in this scenario, not the dominant one. Specificity is incorrect because it measures true negatives divided by true negatives plus false positives, capturing how well the model correctly clears healthy patients — again a measure oriented around the negative class and false positives, not around catching every real tumor case, so it does not directly address the danger of a missed diagnosis. Mean absolute error is incorrect because it is a regression metric measuring the average magnitude of numeric prediction errors; it has no direct application to a binary screening decision like tumor-present versus tumor-absent.
The broader principle to remember: in any high-stakes screening or safety-critical detection task where a missed positive case is dangerous or costly (medical diagnosis, fraud detection where fraud must be caught, safety system failures), recall should be the metric prioritized and often set as the primary target during threshold tuning, even if it means accepting a somewhat lower precision and more false positives, because the asymmetric cost of a missed positive outweighs the cost of extra follow-up on a healthy case.